
What if your own immune cells could be trained to recognize and destroy cancer?
This is no longer a futuristic idea—it’s happening right now.
In 2017, the U.S. Food and Drug Administration approved CAR T-cell therapy, a groundbreaking treatment often described as a “living drug.” Since then, more than 35,000 patients have received it, offering new hope where traditional therapies have failed.
GALLERY OF CAR T-CELL THERAPY IMAGES
How It Works
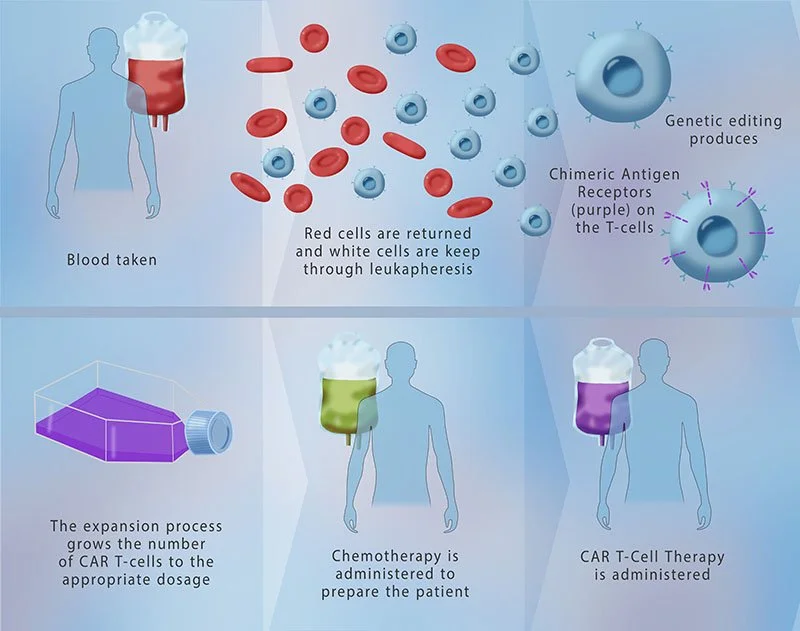
Diagram of the (CAR) T-cell Therapy Process
A diagrammatic illustration of chimeric antigen receptor (CAR) T-cell therapy. The process begins with the extraction of blood from the patient. Through leukapheresis, T-cells are isolated. © Monica Schroeder / Science Source
CAR T-cell therapy harnesses the power of your immune system in a highly personalized way:
First, doctors collect a blood sample and isolate T-cells—white blood cells that play a central role in immune defense. In the lab, these cells are genetically modified to produce Chimeric Antigen Receptors (CARs), which allow them to recognize specific cancer cells.
Once reprogrammed, the cells are multiplied and infused back into the patient’s body. From there, they actively seek out and destroy cancer cells with precision.
A Targeted Approach
A cancer patient's own blood is drawn, modified in a lab, and returned weeks later as a living treatment. It sounds like something out of a near-future film. It's actually standard practice at cancer centers around the world, and it's been since 2017, when the FDA approved the first chimeric antigen receptor (CAR) T-cell therapy, tisagenlecleucel, for a form of pediatric leukemia.
Today there are seven FDA-approved CAR T-cell therapies on the market, covering several types of leukemia, lymphoma, and multiple myeloma. For publishers covering oncology, immunology, or biotechnology, it's one of the more visually compelling stories in modern medicine — and one that depends heavily on good imagery to explain, since the mechanism is almost entirely invisible to the naked eye.
What CAR T-Cell Therapy Actually Does
The "CAR" in CAR T-cell therapy stands for chimeric antigen receptor — chimeric meaning made of parts from different sources, much like the mythological chimera that lent the term its name. That's a fitting description, because the receptor itself is an engineered hybrid: part antibody, part T-cell signaling machinery, stitched together to give an ordinary immune cell a new and very specific job.
The process starts with leukapheresis, a procedure that filters T-cells out of a patient's blood. Those T-cells are sent to a lab, where a disarmed virus is used to insert the gene for the CAR into the cell's DNA. The receptor that results is built to recognize a particular protein on the surface of cancer cells — CD19 on many leukemias and lymphomas, BCMA on multiple myeloma. Once the modified cells are grown into the millions and infused back into the patient, they circulate through the body, latch onto cancer cells displaying that target protein, and trigger their destruction.
It's worth noting how different this is from chemotherapy, which works by killing rapidly dividing cells broadly, healthy and cancerous alike. CAR T-cells are trained for one target. That precision is the whole point, and it's also why the therapy is often called a "living drug" — it isn't a compound that clears the body in hours, but a population of cells that can persist and keep working for years.
A Surprisingly Durable Effect
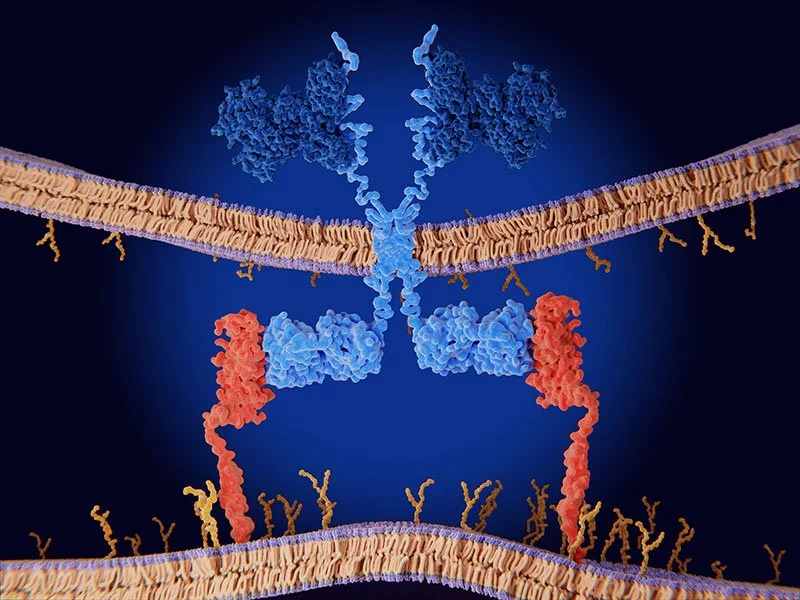
Chimeric antigen receptor (CAR) therapy.
Engineered receptor (light blue) on the surface of a T-lymphocyte bind specifically to CD19-antigen molecules (red) on a leukemia cell. © Juan Gaertner / Science Source
One of the more striking findings to come out of long-term CAR T-cell follow-up studies is just how durable remission can be. Patients in some of the earliest trials, treated more than a decade ago, still have detectable CAR T-cells circulating in their blood and remain cancer-free. That kind of staying power was not a given — many immune therapies fade over time as the engineered cells die off or the body clears them.
Researchers are still working out why some patients respond this way and others don't, which has made CAR T-cell biology one of the more active corners of cancer research. It also explains why this therapy, originally developed for blood cancers, is now being tested far beyond them — in early trials for solid tumors such as glioblastoma and pancreatic cancer, and even in autoimmune diseases like lupus, where the same "seek and destroy" logic is being redirected at malfunctioning immune cells rather than cancer cells.
Why This Story Is Hard to Tell Without the Right Images
CAR T-cell therapy is a genuinely difficult subject to illustrate. There's no tumor to photograph shrinking on a scan, no visible wound, no obvious before-and-after. The actual event being described — a re-engineered T-cell recognizing and binding to a cancer cell — happens at a scale measured in microns. For editors and writers working on this topic, that creates a real gap between the science and what a reader can see.
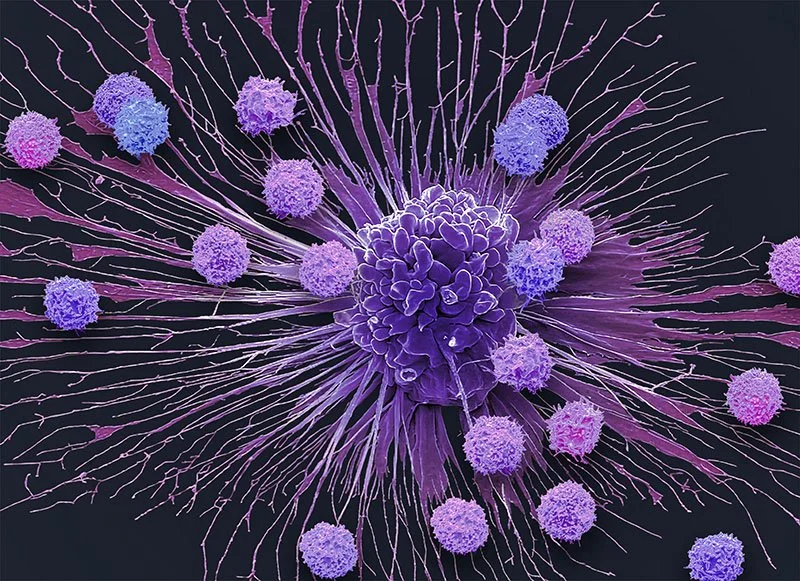
T-cells Surrounding an Apoptotic Hela Cervical Cancer Cell.
Scanning electron micrograph (SEM) of T-cells (small round) and an apoptotic cervical cancer cell (HeLa). T-cells are a component of the body's immune system. © Steve Gschmeissner / Science Source
This is where electron micrographs and medical illustration do work that prose alone can't. A scanning electron micrograph showing a T-cell physically attached to a cancer cell makes the abstract idea of "targeted immune attack" concrete in a way no diagram of arrows and labels really can. A well-rendered 3D illustration of the receptor itself helps readers understand that a CAR isn't a drug in the traditional sense, but a piece of engineered molecular architecture sitting on the surface of a living cell.
Because this is a fast-moving field — new approvals, new targets, expansion into solid tumors and autoimmune disease — publishers also need imagery that won't read as dated or oversimplified next to the current science. Generic "cells under a microscope" stock photography tends to flatten a nuanced mechanism into something generic. Accurate labeling, correct cell morphology, and captions that reflect current terminology matter more here than in most science topics, simply because so few readers (or writers) have a strong mental picture of what a T-cell or a chimeric receptor actually looks like to begin with.
A Field Still Being Written
CAR T-cell therapy isn't a finished story. New CAR designs are in trials that aim to reduce side effects like cytokine release syndrome, "off-the-shelf" allogeneic versions are in development to make treatment faster and cheaper, and researchers are racing to crack the solid-tumor problem that has so far limited this approach mostly to blood cancers. Each of those threads will need its own visual vocabulary as the science evolves — which is part of why an imagery collection in this space needs to be maintained as carefully as the science itself.